






Kabir Abubakar ignored the early signs of malaria in a child under his care, Safiyanu Idris, hoping the illness would pass without treatment.
Mr Abubakar had recently learnt that anti-malaria medicine at the community primary healthcare centre in Yabo, Yauri Local Government Area of Kebbi State, was no longer free. He feared that the treatment would cost more than he could afford, and so, he chose to wait it out.
“Many times, mild symptoms of malaria in children fade without treatment. The sickness in their body just goes away by itself, and I don’t have to worry about anything,” Mr Abubakar said in Hausa.
“I believed it was one of those episodes.”
But Mr Abubakar was wrong. In a few days, Safiyanu’s symptoms worsened. His temperature rose, he struggled to sleep, and could barely sit up. A visit to the town clinic became unavoidable.
Mr Abubakar was met with another surprise when they arrived at the clinic in Yabo. Anti-malaria medicine for his 14-year-old ward was not available. He must purchase them from a pharmacy outside the facility.


Kebbi State, which relied on aid provided through the US Presidential Malaria Initiative (PMI) for the distribution of drugs, was severely affected after the American president, Donald Trump, stopped aid to Nigeria and other countries through an executive order in January last year.
This policy resulted in the dissolution of the United States Agency for International Development (USAID), the country’s key implementing agency.
Since then, malaria drug supply in many parts of Kebbi has declined with many residents struggling to access drugs that were once readily available and freely administered.
Although Nigeria and the US signed, last December, a five-year $5.1 billion Memorandum of Understanding (MoU) for health cooperation aimed at strengthening Nigeria’s health system, improving disease control, and increasing domestic health financing, the implementation will not start until April.
Details of the agreement are yet to be made public and for many Kebbi residents, they are unsure if they will benefit from the new deal.


At the facility in Yabo, drugs are sold to patients once state supplies run out, and when there’s nothing left in the store, patients have to source prescriptions themselves.
For Mr Abubakar, an Islamic teacher with over 50 Almajiris under his care, his pupil’s treatment came at a high cost.
“I didn’t have the money for all the drugs they prescribed, which were also expensive. I had to borrow it.
“Now, I worry about the other boys. They are exposed too, and I cannot afford treatment for them all,” he said.
Anti-malaria at a cost
In many parts of Kebbi, health workers are struggling to provide care to patients with malaria. Drugs are in short supply.
Drugs supply to this facility had been declining for months, Mariya Liman, the senior extension worker at the Yabo town clinic, told PREMIUM TIMES, staring at the empty shelves in the drug store.

According to the Kebbi State Primary Healthcare Development Agency (KSPHCDA), the PMI, through USAID, had been funding the purchase and distribution of malaria drugs to state public health facilities.
It also funded the distribution of mosquito nets and rapid diagnostic tests (RDTs), as well as surveillance and monitoring programmes, for years.
The agency’s malaria elimination programme officer, Nasir Zagga, said the state currently relies on its drug reserve to supply PHCs with malaria medicine, but these are fast running out.
“The quantity of drugs supplied is based on what each facility needs and the number of people they serve. There’s no more funding, and we are trying to manage what we have on the ground. That’s why the quantity of drugs supplied has reduced,” Mr Zagga said.
But health workers who spoke to PREMIUM TIMES disagree with the claim that the drugs provided meet the needs of facilities.
“Drugs run out within the first two weeks after they are supplied,” Ms Liman explained.
“When it is finished, we are forced to buy the drugs ourselves and sell them to patients. We can’t give it for free. How many patients can we help? When we run out of drugs completely, we then ask them to buy.
“That’s why some people think drugs are no longer free. They are still free; they are just not enough.”
A health worker at the Umaru Kare Primary Healthcare Centre in Yelwa, a community neighbouring Yabo, expressed concern about the difference between the number of malaria-positive cases recorded at the facility and the quantity of drugs provided.
“It (drugs supplied) falls significantly short. We get more than 50 positive cases per month, and they supply a few packs of anti-malaria medication once every two months. The difference is vast,” the official said, asking not to be named to avoid victimisation.
Health workers in other parts of the state, including Birnin Kebbi, the state capital, have similar experiences and are worried about their patients.
“Many of the people who visit are those who struggle to pay out of pocket. They can hardly afford necessities, so the availability of free drugs provides crucial relief,” Sheibu Abubakar, the officer-in-charge at the Takalau PHC in Birnin-Kebbi, said.


As the country with the highest burden of malaria globally, malaria is a significant public health concern in Nigeria. The World Health Organisation (WHO) reported an estimated 68 million cases and 194,000 deaths due to the disease in 2021.
In states like Kebbi, where the disease is most prevalent, the risk of transmission persists year-round.
Decline in drug supply
To understand the decline in drug supply and test kits, which health workers complained about at all the PHCs visited, PREMIUM TIMES reviewed the quantities available at some facilities since the announced 90-day stop-work order that eventually led to the dissolution of USAID.
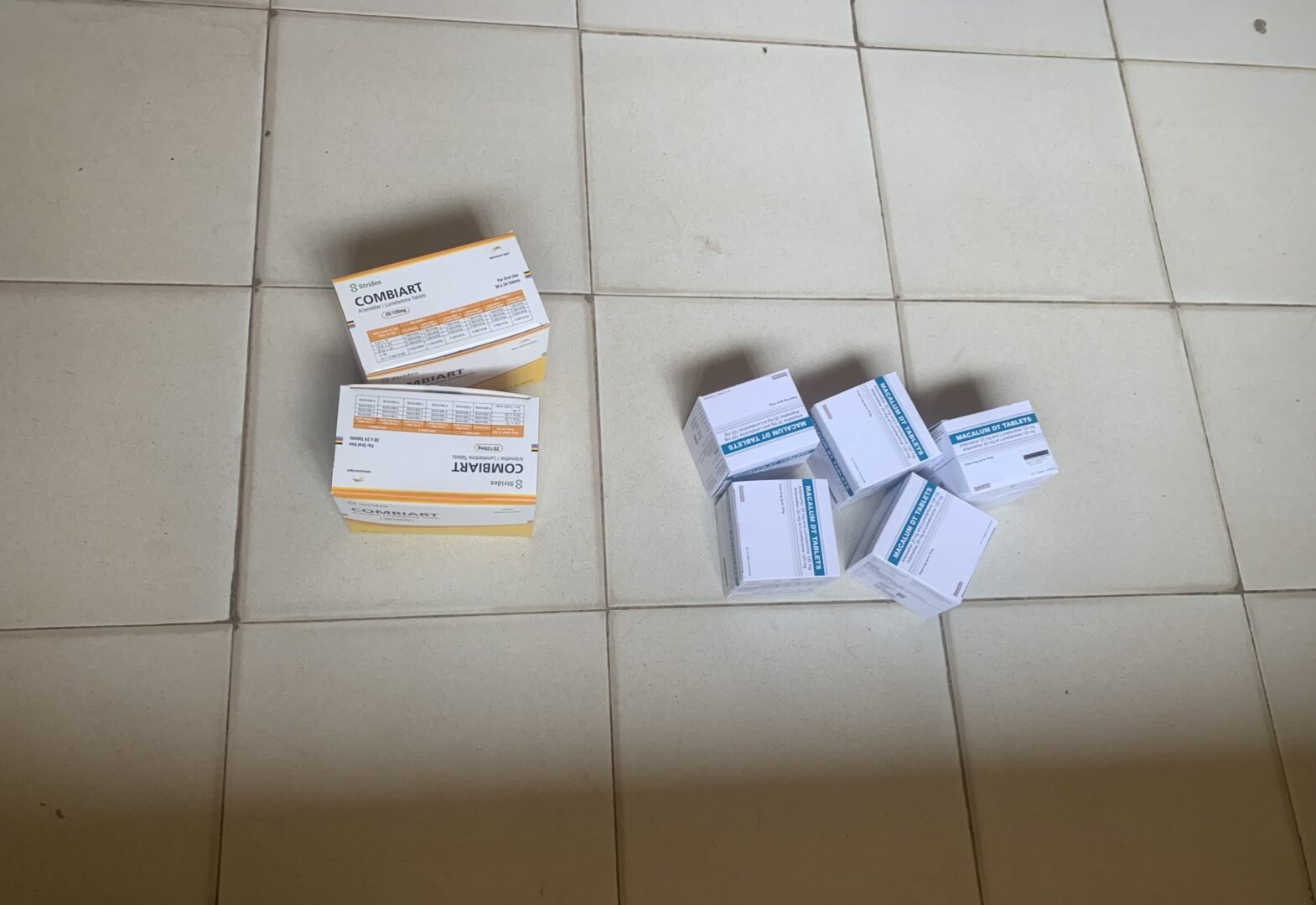
This paper found that Artemisinin-based Combination Therapy (ACT), the standard treatment for malaria in Nigeria, and the Rapid Diagnostic Test (RDT) are supplied to each facility every two months. These drugs come in different doses for adults and children of various age groups.
The ACT medicines are categorised into four groups – ACT 1, 2, 3, and 4. Each is designed for a specific age group.
ACT 1 is given to infants aged 0–1 year, ACT 2 to children aged 1–6 years, ACT 3 to older children aged 7–13 years, and ACT 4 to adults and teenagers aged 14 years and above.
Although the dosages differ, all contain the same Artemisinin-based Combination Therapy used to treat malaria effectively across all age groups.
The town clinic in Yabo received four packs of ACT 1 and received its first ACT supplies after the aid suspension in March 2025. That month, it received four packs of ACT 1, one pack of ACT 2, three packs of ACT 3, 18 packs of ACT 4, and 37 packs of RDTs.
According to Yusuf Swafa, the clinic’s programme officer, the quantity supplied in the last month of the previous year was at least twice that of March.
“The RDT, for instance, was about 50 packs. Usually, RDT packs are stacked in two cartons, but this time, we got only one,” he said.
In May 2025, the clinic only received four packs of ACT 1 and two packs of ACT 4. ACT 2 and 3 were not supplied. RDTs (test kits) were also reduced to around 20 packs.
The supplies remained low in July 2025. Then, in September 2025, the clinic got drugs, but did not receive any test kits, and up until October, there were no test kits at the clinic.
Even after this, supplies did not improve, according to Mr Swafa. It dropped consistently till February 2026.
In November, the clinic received 60 packs of RDTs, nine packs of ACT 2 and 10 packs of ACT 3. ACTs 1 and 4 were not provided.
Then in January, it received fewer than seven packs each of ACT 1, 2, and 3, along with just one pack of RDT.
Unlike the town clinic, the PHC in Nasarawa community, Birnin Kebbi, received its first drugs in February 2025. Then it got four packs of ACT 1, 10 of ACT 2, 13 of ACT 3, and 8 of ACT 4.
By April, the ACT 2 and 3 supplies had fallen to four and six packs, respectively. Between May and June 2025, only five packs of ACT boxes were available. A similar quantity of drugs was also supplied to the clinic between September and November.
The clinic’s supervisor, Hauwa Adamu, told PREMIUM TIMES that supplies remained low since then.
Inconsistent drug supply
Meanwhile, for facilities in Argungun LGA of Kebbi State, medical supplies have not only been low but also inconsistent since the aid cut in early 2025.
The Maternal and Child Health Clinic in Nabame community struggled to get supplies in 2025. The first supply came in January and then another in April, followed by a period when it had no anti-malaria drugs.
“We were not receiving drugs at some point. No one could tell why. We tried to get them, reached out many times, but nothing,” Fatimah Isah, the clinic’s chief extension worker, told PREMIUM TIMES.
Ms Isah stated that the clinic did not receive drugs until well into the second half of the year, and while drugs were eventually made available, the clinic did not receive test kits.
“I don’t know why we are no longer supplied with test kits. We’ve been using clinical tests to diagnose malaria patients because we can’t ask them to buy RDT kits. It’s very expensive,” she said.
“Help us ask the government why they won’t give us test kits. We don’t know why. Help us find out why,” she added.
Meanwhile, malaria contributes substantially to maternal mortality in Kebbi and other parts of Nigeria. According to this study, it accounts for about 11 per cent of maternal deaths in the country.

Mr Zagga, the state malaria elimination programme officer, warned that the situation is likely to worsen over time.
He warned that Kebbi may run out of drugs by the end of the year and would not be able to meet the needs of its population if adequate alternatives are not made.
“The drugs being distributed now are from what we have in store. That’s why we have fewer facilities. We are trying to extend availability for as long as possible. We still have drugs now, but by the end of the year, if we do not make alternatives, things will get worse,” he said.
IDPs struggle for care.
The US aid withdrawal had a jarring impact on many other states because Nigeria was one of the largest recipients of USAID support, and its programmes covered every state across the country.
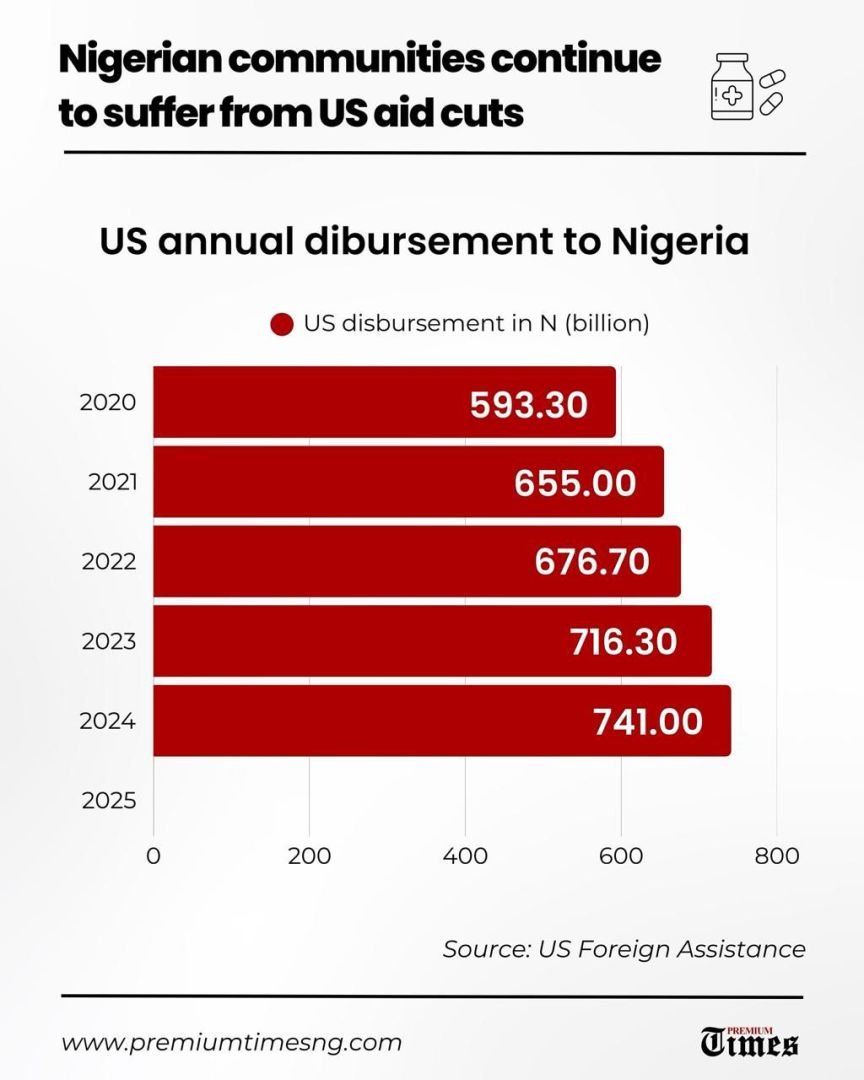
In 2024, Nigeria received about N1.3 trillion in foreign assistance from the US, making it the third-largest African beneficiary that year.
In 2020, the US disbursed N593 billion to Nigeria’s health sector, then N655 billion in 2021. Between 2022 and 2023, it disbursed N677 billion and N716 billion, respectively. In 2024, it disbursed N741 billion.

For malaria control, the US funded interventions through the PMI in at least 11 states, including Kebbi, Benue and Zamfara. All these states were affected by the aid cut.
Shortly after the 90-day stop-work order was announced, the PHC next to the Dauda II Internally Displaced Persons camp in Guma LGA of Benue State was closed and remained shut until the last week of May 2025.
The clinic served the health needs of the over 500 IDPs in the camp, many of whom have been displaced for more than five years.
While the clinic was closed, IDPs were forced to pay out of pocket for healthcare.

Joy Aondongu, 25, recalled visiting a nearby pharmacy when her three-year-old son fell ill with malaria. It was the same pharmacy that many other IDPs turned to for treatment, as there was no functioning PHC nearby.
She told PREMIUM TIMES that she could not afford complete treatment at once and had to save money from her firewood business to buy the drugs gradually.
The clinic had spared her, like many others in the camp, the heavy financial burden of healthcare.
When the clinic eventually reopened months later, much to the relief of everyone, she found that much had changed.
Only one of the three doctors who had previously worked there returned, and getting care had become noticeably slower.
Patients now have to wait in long queues before receiving medical care.
“People now have to wait for longer than one hour before they get to their turn,” she explained.
Increase in drug prices
The health worker at the facility, Israel Wasem, is concerned about the sustainability of the clinic’s operations.
PREMIUM TIMES gathered that the clinic had been established with funding from USAID through the United Nations Children’s Fund (UNICEF). After the aid suspension and USAID’s subsequent dissolution, funding for the clinic dropped significantly.
“The facility used to have other intervention programmes, but right now, there’s only one. You can see the crowd outside, waiting in line for only one doctor. That has been a huge challenge,” Mr Wasem said.
“There has been a decline in drugs. Earlier, UNICEF funded both drugs and payment of staff, but now, we have to rely on the government to supply drugs.”
Joseph Grace, a health worker at the PHC in Ichwa, Makurdi, also indicated that the volume of medical supplies delivered to the facility has steadily declined. Each new shipment arrives with fewer items than the last.
As essential medical commodities become increasingly scarce, frontline health workers struggle to provide care.
Meanwhile, in Kebbi, the prices of drugs have shot up in pharmacies. PREMIUM TIMES visited multiple pharmacies, which said the changes occurred after USAID’s dissolution.
Mr Zagga, the state malaria elimination programme officer, explained to PREMIUM TIMES that, aside from funding drug supplies to health facilities across the state, USAID also subsidised the cost of drugs sold in pharmacies, resulting in cheaper drugs for residents.
After the USAID dissolution, the funding for this stopped, and the price of drugs rose.
“USAID was the reason malaria drugs were cheaper in the state, and when they left, they took their funding with them,” he said.
“The government has allocated some sum,” he said, unwilling to provide more details. “But it is only a fraction of the funding the state was receiving in the form of foreign assistance over the years.
“So much in the past depended on this. If this continues, it will only get worse. Kebbi is really suffering due to the aid withdrawal,” he added. “Truly, we are seriously affected.”
This reporting was completed with the support of the Centre for Journalism Innovation and Development (CJID)
Read the full article here









